
Due to the physiology of the eye [Figure 1], humans experience diminished vision in low-light conditions. Because vision involves the eyes and brain working together, understanding eye function leads to pilot behaviors that can improve night vision significantly.
Anatomy of the Eye
- Light from an object enters the eye through the cornea and then continues through the pupil.
- The opening (dilation) and closing (constriction) of the pupil is controlled by the iris, which is the colored part of the eye. The function of the pupil is similar to that of the diaphragm of a photographic camera: to control the amount of light.
- The lens is located behind the pupil and its function is to focus light on the surface of the retina.
- The retina is the inner layer of the eyeball that contains photosensitive cells called rods and cones. The function of the retina is similar to that of the film in a photographic camera: to record an image.
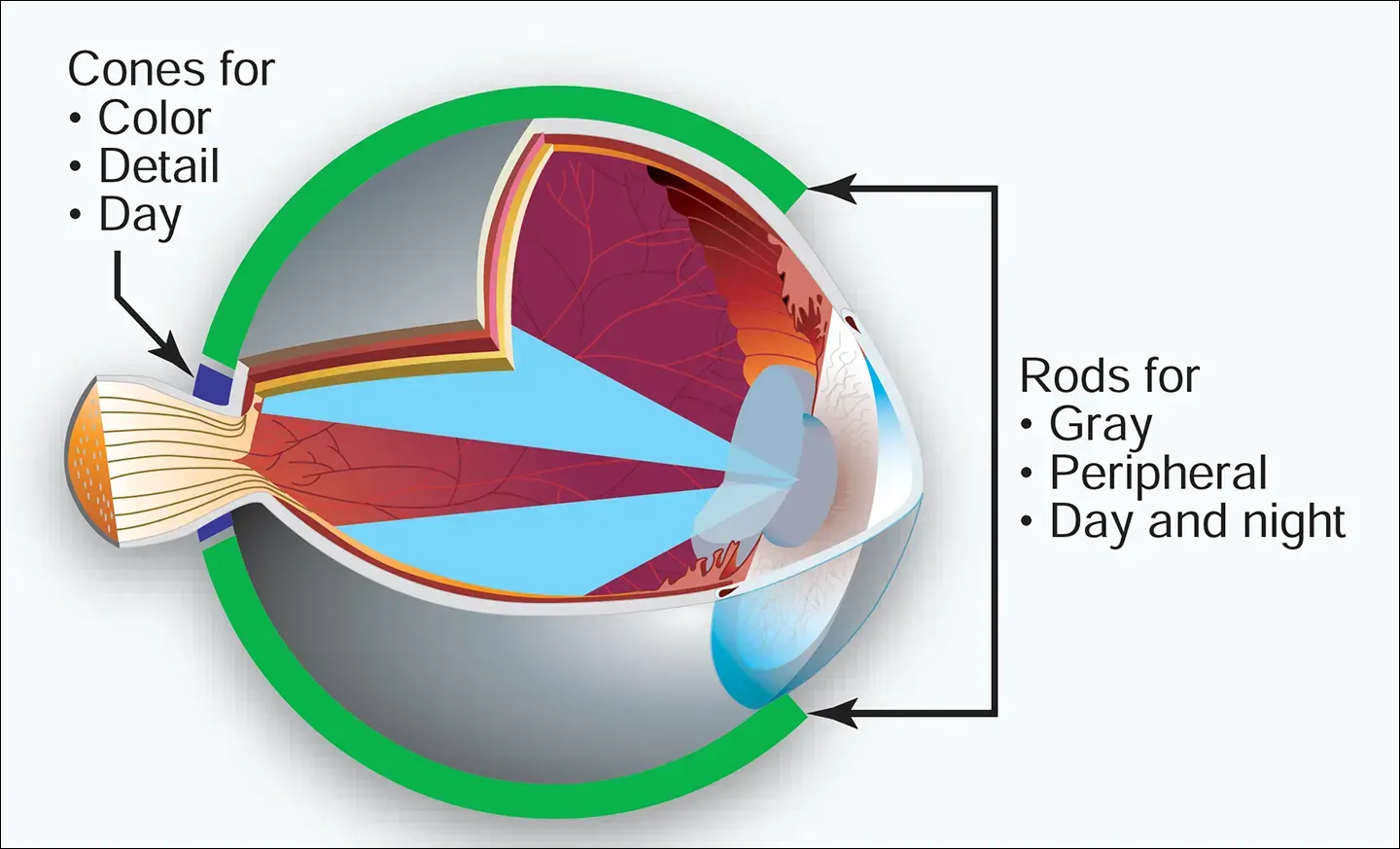
- The cones are located in higher concentrations than rods in the central area of the retina known as the macula, which measures about 4.5 mm in diameter. The exact center of the macula has a very small depression called the fovea, which contains cones only. The cones are used for day or high-intensity light vision. They are involved with central vision to detect detail, perceive color, and identify far-away objects.
- The rods are located mainly in the periphery of the retina—an area that is about 10,000 times more sensitive to light than the fovea. Rods are used for low light intensity or night vision and are involved with peripheral vision to detect position references, including objects (fixed and moving) in shades of gray, but cannot be used to detect detail or to perceive color.
- Although there is not a clear-cut division of function, the rods make night vision possible. The rods and cones function in daylight and in moonlight, but in the absence of normal light, the process of night vision is placed almost entirely on the rods.
- Light energy (an image) enters the eyes and is transformed by the cones and rods into electrical signals that are carried by the optic nerve to the posterior area of the brain (occipital lobes). This part of the brain interprets the electrical signals and creates a mental image of the actual object that was seen by the person.
https://aircraftsystemstech.com/humix/video/UIWeIoRjlIf
Types of Vision
Photopic Vision
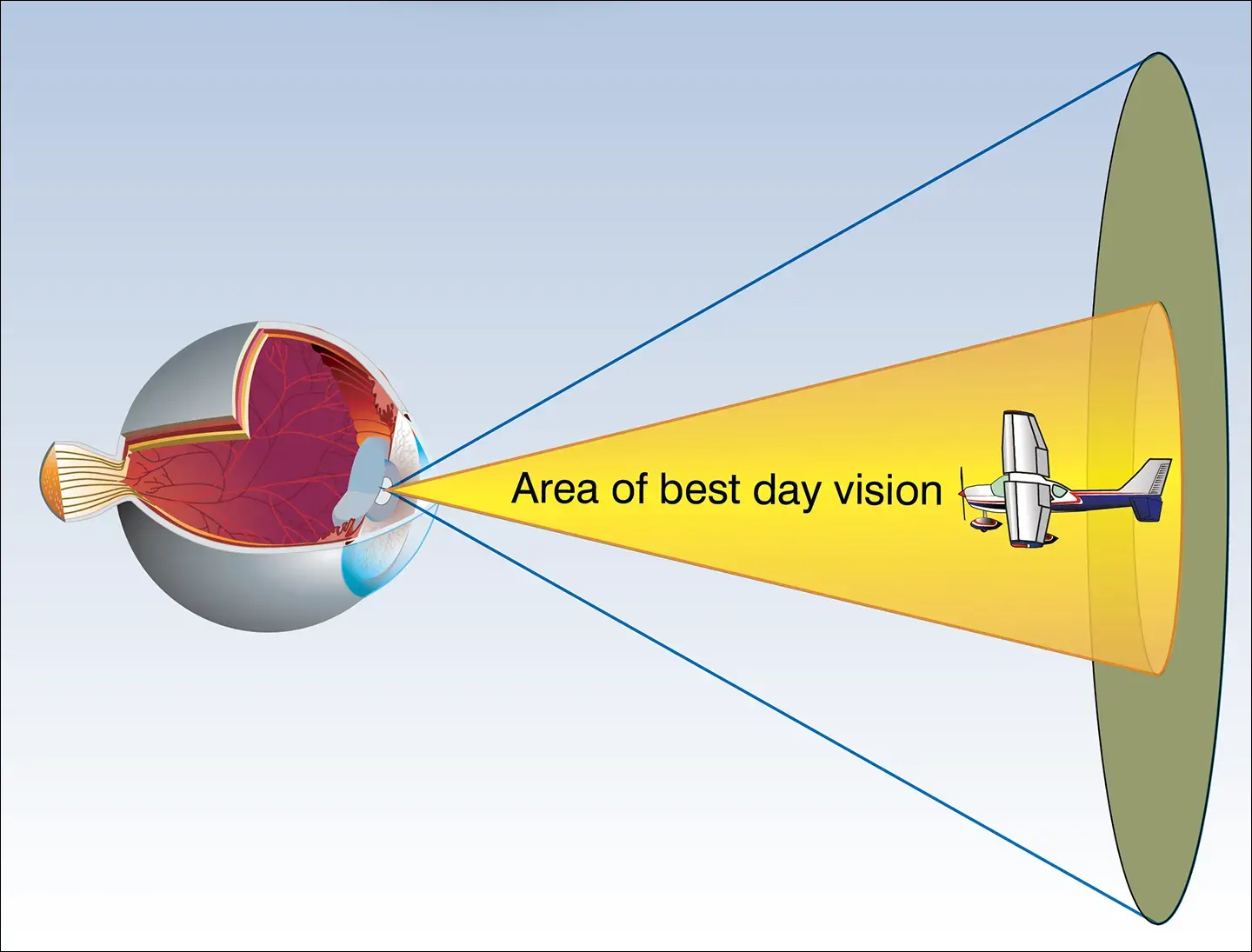
During daytime or high-intensity artificial illumination conditions, the eyes rely on central vision (foveal cones) to perceive and interpret sharp images and color of objects. [Figure 2]
Mesopic Vision
Occurs at dawn, dusk, or under full moonlight levels and is characterized by decreasing visual acuity and color vision. Under these conditions, a combination of central (foveal cones) and peripheral (rods)vision is required to maintain appropriate visual performance.
Scotopic Vision
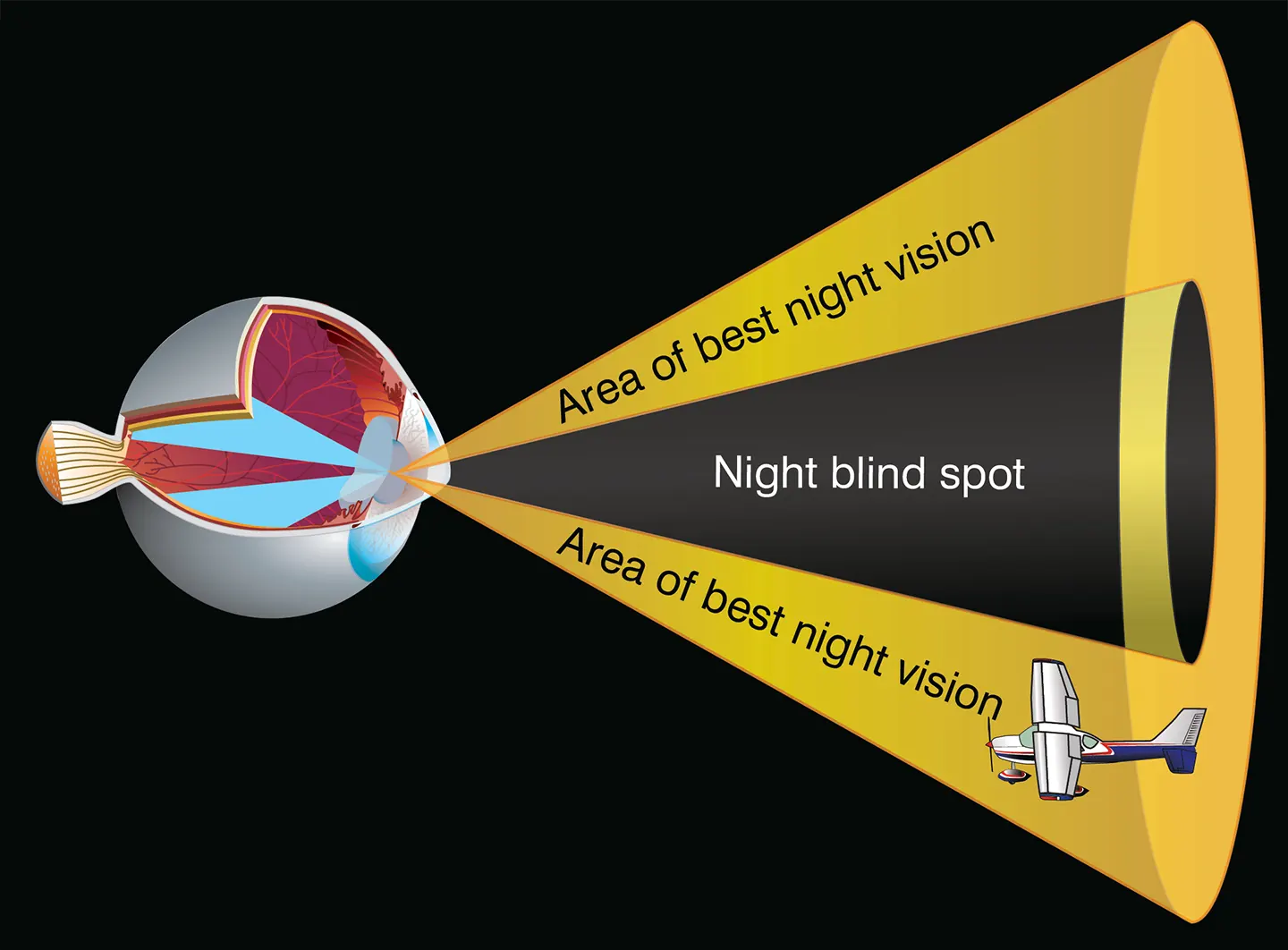
During nighttime, partial moonlight, or low intensity artificial illumination conditions, central vision (foveal cones) becomes ineffective to maintain visual acuity and color perception. Under these conditions, if looking directly at an object for more than a few seconds, the image of the object fades away completely (night blind spot). Peripheral vision (off center scanning) provides the only means of seeing very dim objects in the dark.
Night Blind Spot
The “Night Blind Spot” appears under conditions of low ambient illumination due to the absence of rods in the fovea. [Figure 3] This absence of rods affects the central 5 to 10 degrees of the visual field. If an object is viewed directly at night, it may go undetected or it may fade away after initial detection. The night blind spot can hide larger objects as the distance between the pilot and an object increases.
Vision Under Dim and Bright Illumination
The eye’s adaptation to darkness is another important aspect of night vision. When a dark room is entered, it is difficult to see anything until the eyes become adjusted to the darkness. Almost everyone experiences this when entering a darkened movie theater.
In darkness, vision gradually becomes more sensitive to light. Maximum dark adaptation can take up to 30 minutes. Exposure to aircraft anti-collision lights does not impair night vision adaptation because the intermittent flashes have a very short duration (less than 1 second). However, if dark-adapted eyes are exposed to a bright light source (searchlights, landing lights, flares, etc.) for a period of 1 second or more, night vision is temporarily impaired. If it is safe to do so, pilots may close one eye when bright exposure begins in order to preserve dark adaptation for that eye.
Factors Affecting Vision
- During the day, identification of objects at a distance is aided by good resolution. At night, the identification range of dim objects is limited and the detail resolution is poor.
- Surface references or the horizon may become obscured by smoke, fog, smog, haze, dust, ice particles, or other phenomena, even when visibility meets Visual Flight Rule (VFR) minimums. This is especially true at airports located adjacent to large bodies of water or sparsely populated areas where few, if any, surface references are available. Lack of horizon or surface reference is common on over-water flights, at night, and in low-visibility conditions.
- Presence of uncorrected refractive eye disorders such as myopia (nearsightedness–impaired focusing of distant objects), hyperopia (farsightedness–impaired focusing of near objects), astigmatism (impaired focusing of objects in different meridians), or presbyopia (impaired focusing of near objects) affect day and night vision.
- Self-imposed stresses such as self-medication, alcohol consumption (including hangover effects), tobacco use (including withdrawal), hypoglycemia, sleep deprivation/fatigue, and extreme emotional upset can seriously impair vision.
- Inflight exposure to low barometric pressure without the use of supplemental oxygen (above 10,000 feet during the day and above 5,000 feet at night) can result in hypoxia, which impairs visual performance.
- Due to the effects of carbon monoxide on the blood, smokers may experience a physiological altitude that is much higher than actual altitude. The smoker is thus more susceptible to hypoxia at lower altitudes than the nonsmoker.
- Other factors that may have an adverse effect on visual performance include windscreen haze, improper illumination of the flight deck and/or instruments, scratched and/or dirty instrumentation, use of flight deck red lighting, inadequate flight deck environmental control (temperature and humidity), inappropriate sunglasses and/or prescription glasses/contact lenses, and sustained visual workload during flight. Red light illumination distorts colors (magenta and yellow pigments both appear as red, and cyan pigment appears black) on aeronautical charts. Pilots should use it only where optimum outside night vision capability is necessary. Dim white flight deck lighting should be available when needed for map and instrument reading.
- Monovision contact lenses (one contact lens for distant vision and the other lens for near vision) make the pilot alternate his/her vision; that is, a person uses one eye at a time, suppressing the other, and consequently impairs binocular vision and depth perception. The FAA recommends not using these lenses when piloting an aircraft..
- A flickering light in the flight deck, anti-collision lights, or other aircraft lights, may cause interference with brain function. Although rare, this may occur at a frequencies from 1 to 20 hertz. If continuous, the possible physical reactions can be nausea, dizziness, grogginess, unconsciousness, headaches, or confusion. Pilots should try to eliminate or screen out any light source that might cause an unwanted reaction to blinking or flickering lights.
- Sunglasses can aid the dark adaptation process, which is delayed by prolonged exposure to bright sunlight.